South Thames Retrieval Service in London, UK, provides paediatric intensive care support and retrieval to 2 million children in South East England. During a period of 10 days in mid-April, 2020, we noted an unprecedented cluster of eight children with hyperinflammatory shock, showing features similar to atypical Kawasaki disease, Kawasaki disease shock syndrome, or toxic shock syndrome (typical number is one or two children per week). This case cluster formed the basis of a national alert.
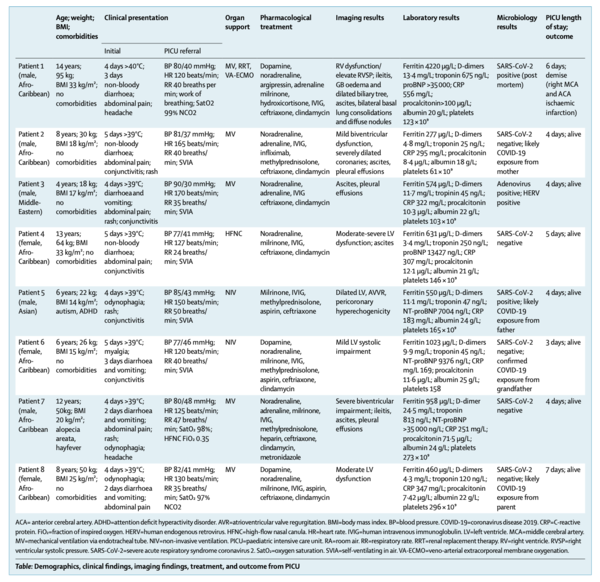
All children were previously fit and well. Six of the children were of Afro-Caribbean descent, and five of the children were boys. All children except one were well above the 75th centile for weight. Four children had known family exposure to coronavirus disease 2019 (COVID-19). Demographics, clinical findings, imaging findings, treatment, and outcome for this cluster of eight children are shown in the table.
Clinical presentations were similar, with unrelenting fever (38-40°C), variable rash, conjunctivitis, peripheral oedema, and generalised extremity pain with significant gastrointestinal symptoms. All progressed to warm, vasoplegic shock, refractory to volume resuscitation and eventually requiring noradrenaline and milrinone for haemodynamic support. Most of the children had no significant respiratory involvement, although seven of the children required mechanical ventilation for cardiovascular stabilisation. Other notable features (besides persistent fever and rash) included development of small pleural, pericardial, and ascitic effusions, suggestive of a diffuse inflammatory process.
All children tested negative for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) on broncho-alveolar lavage or nasopharyngeal aspirates. Despite being critically unwell, with laboratory evidence of infection or inflammation including elevated concentrations of C-reactive protein, procalcitonin, ferritin, triglycerides, and D-dimers, no pathological organism was identified in seven of the children. Adenovirus and enterovirus were isolated in one child.
Baseline electrocardiograms were non-specific; however, a common echocardiographic finding was echo-bright coronary vessels (appendix), which progressed to giant coronary aneurysm in one patient within a week of discharge from paediatric intensive care (appendix). One child developed arrhythmia with refractory shock, requiring extracorporeal life support, and died from a large cerebrovascular infarct. The myocardial involvement in this syndrome is evidenced by very elevated cardiac enzymes during the course of illness.
All children were given intravenous immunoglobulin (2 g/kg) in the first 24 h, and antibiotic cover including ceftriaxone and clindamycin. Subsequently, six children have been given 50 mg/kg aspirin. All of the children were discharged from PICU after 4-6 days. Since discharge, two of the children have tested positive for SARS-CoV-2 (including the child who died, in whom SARS-CoV-2 was detected post mortem). All children are receiving ongoing surveillance for coronary abnormalities.
We suggest that this clinical picture represents a new phenomenon affecting previously asymptomatic children with SARS-CoV-2 infection manifesting as a hyperinflammatory syndrome with multiorgan involvement similar to Kawasaki disease shock syndrome. The multifaceted nature of the disease course underlines the need for multispecialty input (intensive care, cardiology, infectious diseases, immunology, and rheumatology).
The intention of this Correspondence is to bring this subset of children to the attention of the wider paediatric community and to optimise early recognition and management. As this Correspondence goes to press, 1 week after the initial submission, the Evelina London Children's Hospital paediatric intensive care unit has managed more than 20 children with similar clinical presentation, the first ten of whom tested positive for antibody (including the original eight children in the cohort described above).
COVID-19パンデミック時の小児における高炎症性ショック (Lancet 2020.05.07)
英国ロンドンのSouth Thames Retrieval Serviceは、イングランド南東部の200万人の子どもたちに小児集中治療の支援と検索を提供している。我々は2020年4月中旬の10日間の間に、非定型川崎病、川崎病ショック症候群、またはトキシックショック症候群(典型的な数は週に1~2人の子ども)に類似した特徴を示す、高炎症性ショックを呈する8人の子どもたちの前例のないクラスターに気づいた。この症例群は全国的な注意喚起のもととなった。
すべての子供たちは以前は健康であった。このうち6人はアフロ・カリブ系で、5人は男児であった。1人を除くすべての子どもたちは、体重が75パーセンタイル以上であった。4人の小児はコロナウイルス疾患2019(COVID-19)への家族曝露が判明していた。8人の小児のこのクラスタの人口統計学、臨床所見、画像所見、治療、転帰を表に示す。
臨床所見は類似しており、持続的な発熱(38~40℃)、多様な発疹、結膜炎、末梢性浮腫、および顕著な消化器症状を伴う全身性四肢痛を呈していた。すべての小児は末梢熱感を伴う血管弛緩性ショックに進行し、輸液負荷による蘇生に不応性で、最終的にはノルアドレナリンとミルリノンによる血行動態のサポートを必要とした。ほとんどの症例では呼吸器への影響は認められなかったが、7人の症例では心血管の安定化のために人工呼吸器が必要であった。その他の注目すべき特徴は(持続的な発熱と発疹のほかに)、びまん性炎症過程を示唆する少量の胸水、心膜水、腹水の発生であった。
気管支肺胞洗浄液または鼻咽頭吸引液の検査で、重症急性呼吸器症候群コロナウイルス2(SARS-CoV-2)はすべての小児で陰性であった。C 反応性蛋白、プロカルシトニン、フェリチン、トリグリセリド、D-ダイマーの濃度上昇を含む感染または炎症の臨床的証拠があり、重篤な状態であったにもかかわらず、7 人の子供のうち 7人には病理学的生物は確認されなかった。アデノウイルスとエンテロウイルスが1人の子供に分離された。
ベースラインの心電図は非特異的であったが、一般的な心エコー所見はエコーブライトな冠血管であり(appendix)、小児集中治療から退院後1週間以内に1人の患者で巨大冠動脈瘤に進行した(appendix)。1例の小児は難治性ショックを伴う不整脈を発症し、ECMOを必要とし、大脳血管梗塞で死亡した。この症候群における心筋の関与は、疾患の経過中の心臓酵素の非常に高い上昇によって証明されている。
すべての小児に最初の24時間に免疫グロブリン(2g/kg)を静脈内投与し、セフトリアキソンとクリンダマイシンを含む抗生物質のカバーを行った。その後、6人の子供には50mg/kgのアスピリンが投与された。4-6日後に全児がPICUから退院した。退院後、2名の小児がSARS-CoV-2の陽性反応を示した(死亡した小児を含め、死後にSARS-CoV-2が検出された)。すべての小児は冠動脈異常のサーベイランスを継続的に受けている。
この臨床像は,これまで無症状であったSARS-CoV-2感染児が川崎病ショック症候群に類似した多臓器に侵襲を伴う炎症性亢進症候群を呈する新たな現象であることを示唆している.。患経過が多面的であることから、多職種(集中治療科、循環器科、感染症科、免疫科、リウマチ科)の協力が必要であることが明らかになった。
この報告の意図は、このサブセットの子供たちをより広い小児科コミュニティの注目を集め、早期の認識と管理を最適化することである。本報告が発行されてから1週間後、エヴェリナロンドン小児病院小児集中治療室では、同様の臨床症状を呈する20人以上の小児を管理しており、そのうち最初の10人が抗体陽性となった(上記のコホートに含まれていた8人の小児を含む)。
(Smart119 スタッフコメント)
小児重症例の報告。川崎病に類似した症状を呈し、炎症亢進を認めている。
https://www.thelancet.com/action/showPdf?pii=S0140-6736%2820%2931094-1