Key Points
Question
Is administration of systemic corticosteroids associated with reduced 28-day mortality in critically ill patients with coronavirus disease 2019 (COVID-19)?
Findings
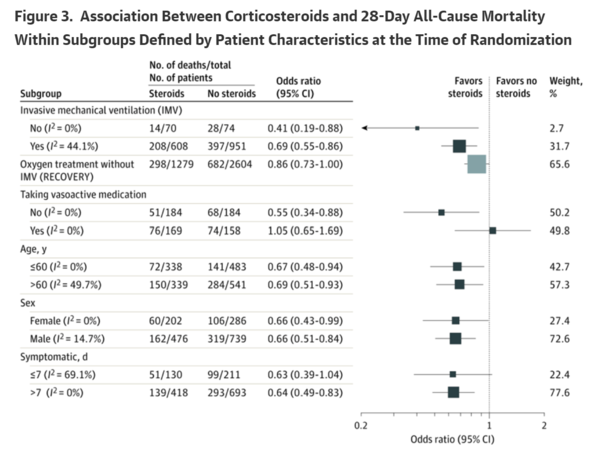
In this prospective meta-analysis of 7 randomized trials that included 1703 patients of whom 647 died, 28-day all-cause mortality was lower among patients who received corticosteroids compared with those who received usual care or placebo (summary odds ratio, 0.66).
Meaning
Administration of systemic corticosteroids, compared with usual care or placebo, was associated with lower 28-day all-cause mortality in critically ill patients with COVID-19.
Abstract
Importance
Effective therapies for patients with coronavirus disease 2019 (COVID-19) are needed, and clinical trial data have demonstrated that low-dose dexamethasone reduced mortality in hospitalized patients with COVID-19 who required respiratory support.
Objective
To estimate the association between administration of corticosteroids compared with usual care or placebo and 28-day all-cause mortality.
Design, Setting, and Participants
Prospective meta-analysis that pooled data from 7 randomized clinical trials that evaluated the efficacy of corticosteroids in 1703 critically ill patients with COVID-19. The trials were conducted in 12 countries from February 26, 2020, to June 9, 2020, and the date of final follow-up was July 6, 2020. Pooled data were aggregated from the individual trials, overall, and in predefined subgroups. Risk of bias was assessed using the Cochrane Risk of Bias Assessment Tool. Inconsistency among trial results was assessed using the I2 statistic. The primary analysis was an inverse variance-weighted fixed-effect meta-analysis of overall mortality, with the association between the intervention and mortality quantified using odds ratios (ORs). Random-effects meta-analyses also were conducted (with the Paule-Mandel estimate of heterogeneity and the Hartung-Knapp adjustment) and an inverse variance-weighted fixed-effect analysis using risk ratios.
Exposures
Patients had been randomized to receive systemic dexamethasone, hydrocortisone, or methylprednisolone (678 patients) or to receive usual care or placebo (1025 patients).
Main Outcomes and Measures
The primary outcome measure was all-cause mortality at 28 days after randomization. A secondary outcome was investigator-defined serious adverse events.
Results
A total of 1703 patients (median age, 60 years [interquartile range, 52-68 years]; 488 [29%] women) were included in the analysis. Risk of bias was assessed as "low" for 6 of the 7 mortality results and as "some concerns" in 1 trial because of the randomization method. Five trials reported mortality at 28 days, 1 trial at 21 days, and 1 trial at 30 days. There were 222 deaths among the 678 patients randomized to corticosteroids and 425 deaths among the 1025 patients randomized to usual care or placebo (summary OR, 0.66 [95% CI, 0.53-0.82]; P < .001 based on a fixed-effect meta-analysis). There was little inconsistency between the trial results (I2 = 15.6%; P = .31 for heterogeneity) and the summary OR was 0.70 (95% CI, 0.48-1.01; P = .053) based on the random-effects meta-analysis. The fixed-effect summary OR for the association with mortality was 0.64 (95% CI, 0.50-0.82; P < .001) for dexamethasone compared with usual care or placebo (3 trials, 1282 patients, and 527 deaths), the OR was 0.69 (95% CI, 0.43-1.12; P = .13) for hydrocortisone (3 trials, 374 patients, and 94 deaths), and the OR was 0.91 (95% CI, 0.29-2.87; P = .87) for methylprednisolone (1 trial, 47 patients, and 26 deaths). Among the 6 trials that reported serious adverse events, 64 events occurred among 354 patients randomized to corticosteroids and 80 events occurred among 342 patients randomized to usual care or placebo.
Conclusions and Relevance
In this prospective meta-analysis of clinical trials of critically ill patients with COVID-19, administration of systemic corticosteroids, compared with usual care or placebo, was associated with lower 28-day all-cause mortality.
COVID-19の重症患者における全身副腎皮質ステロイド投与と死亡率の関連性 メタアナリシス(JAMA 2020.09.02)
要点
疑問
全身副腎皮質ステロイドの投与は、COVID-19の重症患者における28日死亡率の低下と関連しているか?
所見
1703人の患者を対象とした7つの無作為化試験に対する今回の前向きメタアナリシスでは、647人が死亡したが、副腎皮質ステロイドを投与された患者では、通常の治療を受けた患者やプラセボを投与された患者と比較して、28日間の全死因死亡率が低かった(要約オッズ比、0.66)。
意義
COVID-19の重症患者において、通常の治療やプラセボと比較して、全身副腎皮質ステロイドの投与は、28日間の全死亡率の低下と関連していた。
抄録
重要性
COVID-19患者に対する有効な治療法が必要とされており,呼吸補助を必要とするCOVID-19入院患者において、低用量デキサメタゾンが死亡率を減少させることが臨床試験データで示されている。
目的
通常の治療またはプラセボと比較した、副腎皮質ステロイド投与と28日間の全死因死亡率との関連を推定すること。
デザイン、設定、および参加者
COVID-19の重症患者1703例を対象に、副腎皮質ステロイドの有効性を評価した7つの無作為化臨床試験のデータをプールした前向きメタアナリシス。試験は2020年2月26日から2020年6月9日まで12カ国で実施され、最終追跡日は2020年7月6日とした。プールされたデータは、個々の試験、全体、および事前に定義されたサブグループで集計した。バイアスのリスクはコクランの評価ツールを用いて評価した。試験結果間の不整合は、I2 統計量を用いて評価した。一次解析は全死亡率の逆分散加重固定効果メタアナリシスで、介入と死亡率との関連をオッズ比(OR)を用いて定量化した。ランダム効果メタアナリシスも実施され(不均一性のPaule-Mandel推定値とHartung-Knapp調整を用いて)、リスク比を用いた逆分散加重固定効果分析が行われた。
暴露
患者は、全身デキサメタゾン、ヒドロコルチゾン、またはメチルプレドニゾロンの投与(678例)、または通常の治療かプラセボの投与(1025例)に無作為に割り付けられた。
主要評価項目
主要評価項目は無作為化28日後の全死因死亡であった。副次的評価項目は、研究者が定義した重篤な有害事象であった。
結果
合計1703例(年齢中央値60歳[四分位範囲52~68歳]、488例[29%]が女性)が解析に含まれた。バイアスのリスクは、7つの試験のうち6つの試験では「低い」と評価され、1つの試験では無作為化の方法のために「やや懸念がある」と評価された。28日死亡率が報告された試験が5つ、21日死亡率が報告された試験が1つ、30日死亡率が報告された試験が1つであった。副腎皮質ステロイドに割り付けられた678人の患者のうち死亡は222人、通常の治療またはプラセボに割り付けられた1025人の患者のうち死亡は425人であった(要約OR 0.66[95%信頼区間 0.53-0.82];P<0.001、固定効果メタアナリシスに基づく)。試験結果の間にはほとんど矛盾がなく(I2 = 15.6%;不均一性についてはP = 0.31)、ランダム効果メタアナリシスに基づく要約ORは0.70(95%信頼区間 0.48-1.01;P = 0.053)であった。死亡率との関連についての固定効果要約ORは、通常の治療またはプラセボと比較してデキサメタゾン(3試験、患者数1282人、死亡数527人)では0.64(95%信頼区間 0.50-0.82;P<0.001)であり、 ヒドロコルチゾン(3試験、患者数374人、死亡数94人)では0.69(95%信頼区間 0.43-1.12;P = 0.13)であり、メチルプレドニゾロン(1試験、患者数47人、死亡数26人)では0.91(95%信頼区間 0.29-2.87;P = 0.87)であった。重篤な有害事象が報告された6つの試験のうち、副腎皮質ステロイドに割り付けられた354人の患者で64件、通常の治療またはプラセボに割り付けられた342人の患者で80件が発生した。
結論と関連性
COVID-19の重症患者を対象とした臨床試験に対する今回の前向きメタアナリシスでは、全身副腎皮質ステロイドの投与は、通常の治療やプラセボと比較して、28日間の全死因死亡率の低下と関連していた。