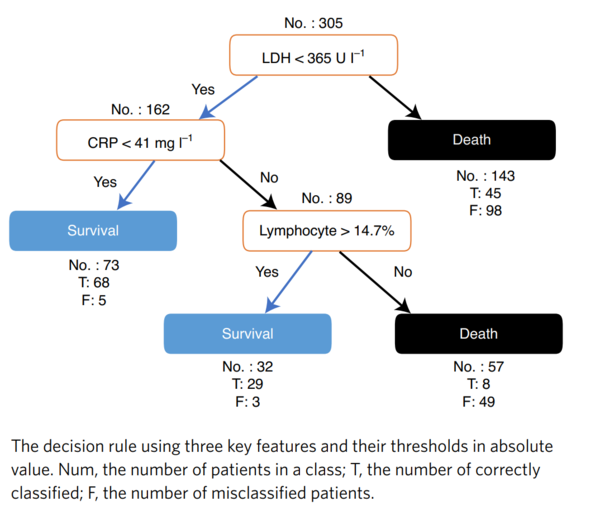
There is a clear need for a simple mortality prediction model to help guide clinical decision making for patients with COVID-19. Yan et al. demonstrated the strong predictive capacity of a decision rule consisting of three readily available laboratory measures for COVID-19 mortality: lactate dehydrogenase (LDH), high-sensitivity C-reactive protein (hs-CRP) and percent lymphocytes.
We performed an independent replication of their model using data from our large general hospital (St Antonius Hospital, Nieuwegein, the Netherlands). We included 305 patients over 18 years of age who presented to the emergency room with a clinical suspicion of COVID-19 between 19 March and 4 May 2020, with a positive SARS-CoV-2 polymerase chain reaction (PCR) result and for whom data for the three biomarkers were available at presentation. Mortality data were collected on 14 May 2020 at an average follow-up duration of 41 days.
The average age of the patients was 62.7 years and 188 (62%) were male. Of these patients, 61 died (at 1-33 days after admission, with a median of 7 days). We found that the model has 92% survival prediction accuracy but only 27% mortality prediction accuracy. This compares to a 100% survival prediction and 81% mortality prediction found by Yan et al.
In our population, 42 out of 303 patients were admitted to the intensive care unit (ICU). Of these patients, 36 (86%) had an unfavourable outcome from the decision rule, but only 15 (36%) of them died (all with LDH > 365 U l−1).
We conclude that, in Dutch patients, a favourable outcome of the decision rule was indeed a good predictor of non-admission to the ICU and of survival. Although an unfavourable outcome of the decision rule could have been interpreted as a warning sign, the majority of our patients thus classified still survived. We hypothesize that this discrepancy between our data and those of Yan et al. may be due to genetic differences in the expression of the presented biomarkers. For example, LDH expression has been reported to display substantial genetic heterogeneity between Asians and Caucasians. Alternatively, differences in treatment protocol or in baseline characteristics of the patients may have influenced the outcome.
In conclusion, our analysis supports the high survival prediction accuracy of the decision rule proposed by Yan et al., but fails to confirm its high mortality prediction accuracy. The identification of patients with COVID-19 with a low risk of mortality can be useful to inform the level of surveillance within or outside the hospital.
COVID-19患者に対して臨床的判断を下すのに役立つ、単純な死亡予測モデルの必要性は明らかである。Yanらは、COVID-19患者の死亡率の予測に関して、乳酸脱水素酵素(LDH)、高感度C反応性蛋白(hs-CRP)、リンパ球率の3つの検査値からなる予測ルールによる強力な予測能力を実証した。
我々は、我々の大規模な総合病院(St Antonius Hospital, Nieuwegein, オランダ)のデータを用いて、彼らのモデルの独立した複製を行った。我々は、2020年3月19日から5月4日までの間に、COVID-19が臨床的に疑われて救急外来に来院し、SARS-CoV-2ポリメラーゼ連鎖反応(PCR)の結果が陽性で、3つのバイオマーカーのデータが提示時に利用可能な18歳以上の患者305人を対象に含めた。死亡データは2020年5月14日に集められ、平均追跡期間は41日であった。
患者の平均年齢は62.7歳で、188人(62%)が男性であった。これらの患者のうち61人が死亡した(入院後1~33日目に死亡、中央値は7日)。このモデルの生存予測精度は92%であるが、死亡予測精度は27%にすぎないことがわかった。これは、Yanらによって発見された100%の生存予測と81%の死亡率予測と比較している。
我々の集団では、303人の患者のうち42人が集中治療室(ICU)に入院した。これらの患者のうち、36人(86%)が予測ルールからは好ましくない転帰を示したが、死亡したのは15人(36%)のみであった(いずれもLDH>365 U l-1)。
我々は、オランダの患者において、予測ルールからの好ましい結果は確かにICU入室の回避と生存に関する良い予測因子であったと結論付けた。予測ルールの好ましくない結果は警告のサインと解釈される可能性があったが、このように分類された患者の大多数は依然として生存していた。我々は、我々のデータとYanらのデータとの間のこの不一致は、提示されたバイオマーカーの発現における遺伝的な違いによるものではないかと仮説を立てた。例えば、LDHの発現はアジア人と白人の間でかなりの遺伝的不均一性を示すことが報告されている。また、治療プロトコルの違いや患者のベースラインの特徴が転帰に影響を与えている可能性もある。
結論として、我々の解析は、Yanらが提案した予測ルールの高い生存予測精度を支持するが、死亡率予測精度の高さを確認するには至らなかった。死亡リスクの低いCOVID-19を有する患者の同定は、院内または院外でのサーベイランスのレベルを知らせるのに有用である。